Introduction
A stroke is a life-threatening medical emergency caused by disruption of blood flow to the brain. This interruption starves brain cells of oxygen and nutrients, leading to tissue damage or death. Strokes are broadly classified into two main types: ischemic stroke, caused by a blockage of blood vessels, and hemorrhagic stroke, caused by bleeding into or around the brain. While both types share some symptoms, their causes, diagnostic pathways, and treatments differ significantly. Understanding these differences is crucial for timely and effective intervention.
1. Ischemic Stroke
Overview
Ischemic stroke accounts for approximately 87% of all strokes worldwide. It occurs when a cerebral artery is blocked, resulting in decreased or absent blood flow to parts of the brain.
Causes
- Atherosclerosis: The most common cause involves plaque buildup (fatty deposits) inside the arteries, narrowing them and leading to clot formation.
- Thrombosis: A blood clot forms at the site of a narrowed artery and obstructs blood flow.
- Embolism: A clot or debris (embolus) formed elsewhere in the body—commonly in the heart during atrial fibrillation—travels through the bloodstream and lodges in a brain artery.
- Other causes: Less common sources include artery dissection, low blood flow states, or hypercoagulable conditions (blood clotting disorders).
Pathophysiology
The blockage results in ischemia (lack of oxygen), causing:
- Energy failure in brain cells
- Loss of ion gradients
- Cell swelling and death (infarction)
- Inflammation and damage to the blood-brain barrier
The brain tissue surrounding the blocked artery, called the ischemic penumbra, is at risk but potentially salvageable with rapid reperfusion.
Symptoms
Ischemic stroke symptoms typically develop suddenly and vary depending on the brain area affected:
- Sudden weakness or numbness on one side of the body (face, arm, or leg)
- Difficulty speaking or understanding language (aphasia)
- Vision problems (blurred or loss of vision in one or both eyes)
- Dizziness, loss of balance or coordination (ataxia)
- Sudden confusion or difficulty swallowing
- Severe headache may occur but is less common than in hemorrhagic stroke
Diagnosis
- Clinical assessment: Neurological exam assessing deficits.
- Imaging:
- Non-contrast CT scan: To exclude hemorrhage and guide treatment. Usually normal in early ischemia.
- MRI (Diffusion-weighted imaging): More sensitive to early ischemic changes.
- CT or MR angiography: To identify blocked vessels.
- Blood tests: Coagulation profile, blood glucose, and cardiac markers.
Treatment
- Acute phase:
- Intravenous thrombolysis: Administration of tissue plasminogen activator (tPA) within 3-4.5 hours of symptom onset to dissolve the clot.
- Mechanical thrombectomy: Catheter-based clot removal, effective up to 24 hours in selected cases.
- Supportive care: Oxygen therapy, blood pressure management, blood sugar control.
- Secondary prevention:
- Antiplatelet therapy (aspirin, clopidogrel) or anticoagulation for atrial fibrillation.
- Statins to reduce cholesterol and stabilize plaques.
- Lifestyle modifications and management of risk factors (hypertension, diabetes, smoking cessation).
2. Hemorrhagic Stroke
Overview
Hemorrhagic stroke constitutes about 13% of strokes but has a higher mortality rate and often results in more severe disability. It is caused by rupture of a blood vessel within the brain or into the surrounding spaces, leading to bleeding and increased intracranial pressure.
Types of Hemorrhagic Stroke
- Intracerebral hemorrhage (ICH): Bleeding occurs directly into the brain tissue. The most common cause is uncontrolled hypertension.
- Subarachnoid hemorrhage (SAH): Bleeding into the subarachnoid space surrounding the brain, often caused by a ruptured aneurysm or arteriovenous malformation (AVM).
Causes
- Hypertension: Chronic high blood pressure weakens small arteries, causing rupture.
- Aneurysm rupture: Weak, bulging areas in artery walls can burst suddenly.
- Arteriovenous malformations: Congenital tangles of abnormal vessels prone to rupture.
- Trauma: Head injury causing vessel damage.
- Bleeding disorders: Including anticoagulant medication overuse or blood clotting abnormalities.
- Amyloid angiopathy: Deposition of amyloid in cerebral vessels, common in the elderly.
Pathophysiology
- Blood leaks into brain tissue or spaces, causing:
- Direct tissue injury
- Compression and displacement of brain structures
- Increased intracranial pressure (ICP)
- Reduced cerebral perfusion pressure
Symptoms
Hemorrhagic stroke symptoms often have a sudden and dramatic onset:
- Sudden severe headache (“worst headache of life” in SAH)
- Nausea and vomiting
- Loss of consciousness or decreased alertness
- Weakness or numbness on one side of the body
- Seizures
- Visual disturbances
- Neck stiffness (in subarachnoid hemorrhage)
Diagnosis
- CT scan: Quick and effective at identifying bleeding.
- MRI: Helpful in some cases to detail bleeding and underlying causes.
- CT or MR angiography: To detect aneurysms or vascular malformations.
- Lumbar puncture: Occasionally used if subarachnoid hemorrhage is suspected but imaging is inconclusive.
Treatment
- Stabilization: Airway management, blood pressure control (usually lowering elevated BP to reduce bleeding risk), and monitoring for increased ICP.
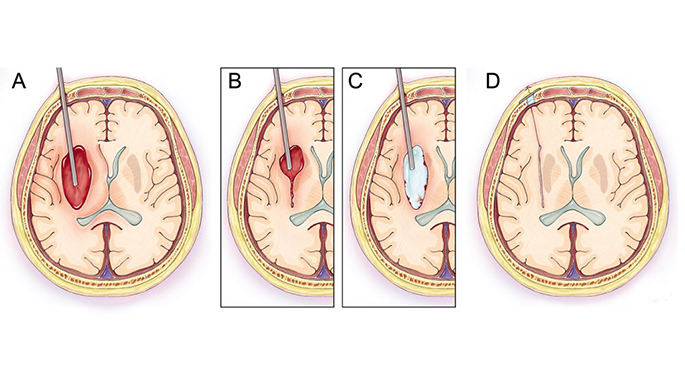
- Surgical interventions:
- Craniotomy to evacuate large hematomas or repair ruptured vessels.
- Endovascular coiling or clipping of aneurysms in SAH.
- Medications:
- Agents to reverse anticoagulation if applicable.
- Medications to control seizures, reduce brain swelling (mannitol, hypertonic saline).
- Supportive care: Intensive monitoring in neurocritical care units.
Key Differences Between Ischemic and Hemorrhagic Stroke
| Feature | Ischemic Stroke | Hemorrhagic Stroke |
| Cause | Blood vessel blockage (clot/thrombus/embolism) | Blood vessel rupture causing bleeding |
| Percentage of strokes | ~87% | ~13% |
| Onset | Sudden, sometimes preceded by TIA | Sudden, often with severe headache |
| Initial imaging | CT shows no bleeding; MRI detects ischemia early | CT shows bleeding immediately |
| Treatment focus | Restore blood flow (thrombolysis, thrombectomy) | Control bleeding, reduce pressure, surgery |
| Risk of death | Lower compared to hemorrhagic | Higher mortality and morbidity |
| Long-term recovery | Variable, often better with early treatment | Often more severe disability, longer rehab |
Prevention of Stroke
Prevention strategies overlap for both types but focus on controlling underlying risk factors:
- Control blood pressure: The most important modifiable risk factor for both ischemic and hemorrhagic stroke.
- Manage diabetes and cholesterol: Reduces risk of atherosclerosis.
- Lifestyle changes: Healthy diet, regular exercise, smoking cessation, limiting alcohol.
- Treat heart conditions: Especially atrial fibrillation with anticoagulants to prevent embolic stroke.
- Avoid illicit drugs, Such as cocaine, which increases stroke risk.
Recovery and Rehabilitation
Post-stroke recovery depends on severity, location, and treatment timing:
- Early physical, occupational, and speech therapy can maximize functional recovery.
- Psychological support is important due to risk of depression.
- Secondary stroke prevention plans are vital to reduce recurrence risk.
Conclusion
Ischemic and hemorrhagic strokes are medical emergencies with distinct causes and treatment pathways. Ischemic stroke, caused by blood clots, is treated primarily with clot-dissolving or removal strategies. Hemorrhagic stroke results from bleeding in the brain, requiring measures to control hemorrhage and relieve pressure. Both require rapid recognition and intervention to reduce brain damage and improve outcomes. Preventive care focused on risk factor management is key to lowering the overall burden of stroke.
FAQs
How are ischemic and hemorrhagic strokes diagnosed so quickly?
Non-contrast CT scans are the first step to distinguish bleeding from blockage, guiding immediate treatment.
Can hemorrhagic stroke follow ischemic stroke?
Yes, ischemic stroke can sometimes convert to hemorrhagic due to damaged blood vessels.
Why can’t thrombolytic drugs be used for hemorrhagic stroke?
Because they thin the blood and increase bleeding, worsening hemorrhage.
What is the role of surgery in stroke?
Surgery is mainly for hemorrhagic stroke to remove blood or repair vessels; thrombectomy is a minimally invasive procedure for ischemic stroke.
How important is timing in stroke treatment?
Every minute counts—early treatment significantly reduces brain damage and improves recovery chances.